

Latest
The Genetic Secrets of Sperm Warfare
How some genes can rig the system




Latest Stories

What Doomsday Prophecies Say About Us
An interview with medieval studies scholar and apocalypse expert Matthew Gabriele

Newly Discovered Species Changes the Origin Story of Magic Mushrooms
There’s a new psychedelic mushroom in town

Psychology
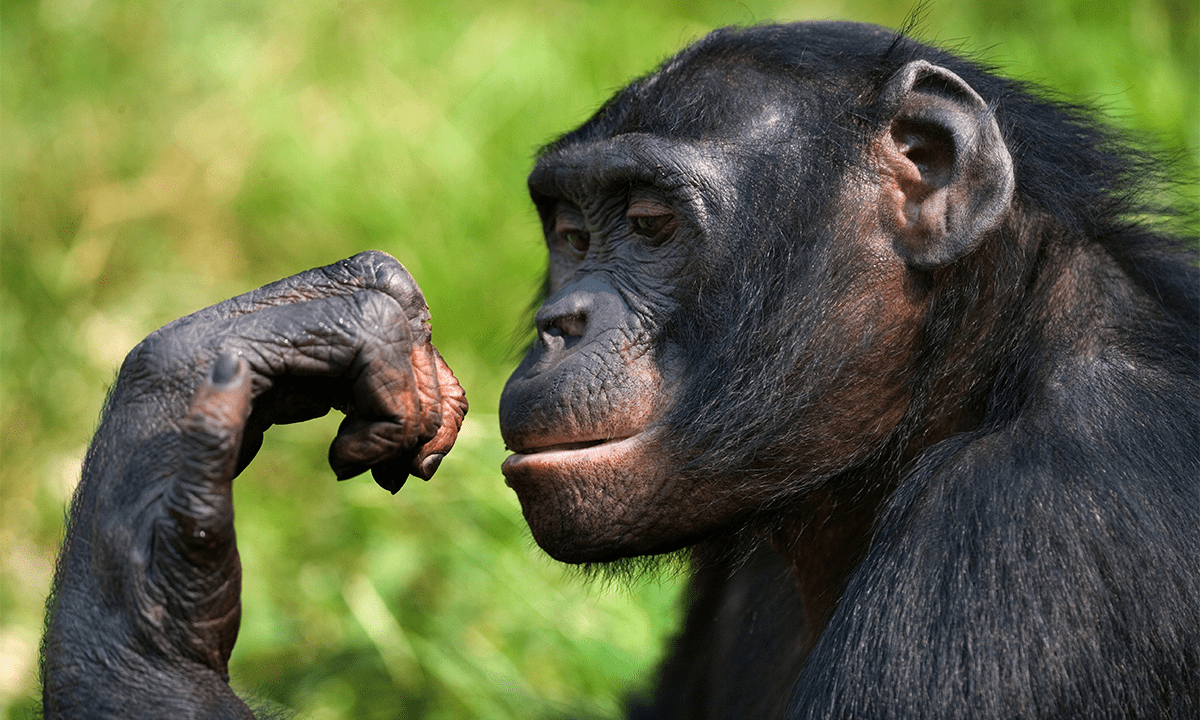
See more PsychologyHumans Can Read the Expressions and Feelings of Our Primate Cousins
Just like our primate cousins can read human expressions

You Can Still Improve as You Age—With the Right Mindset
New research is challenging traditional assumptions of aging
Weed Not Only Sends Memories Up in Smoke, It Reshapes Them
Break out the sticky notes next time you smoke

Environment
See more EnvironmentHow Flowers Transformed Planet Earth
An interview with biologist David George Haskell about his new book

It’s Not Just You. Subways the World Over Are Feeling Hotter
Complaints of extreme heat are rising

The Ancient Cold Snaps That May Have Shaped Human Evolution
Here’s when Earth’s climate became chaotic

Get unlimited, ad-free Nautilus. Become a member today.
History
See more HistoryHow Three Students Designed an Atomic Bomb
A top-secret 1960s project tasked physics postdocs with building The Bomb

The Thrill of Science in 2042
A science historian explains how science got its groove back. A fictional dispatch from the future.
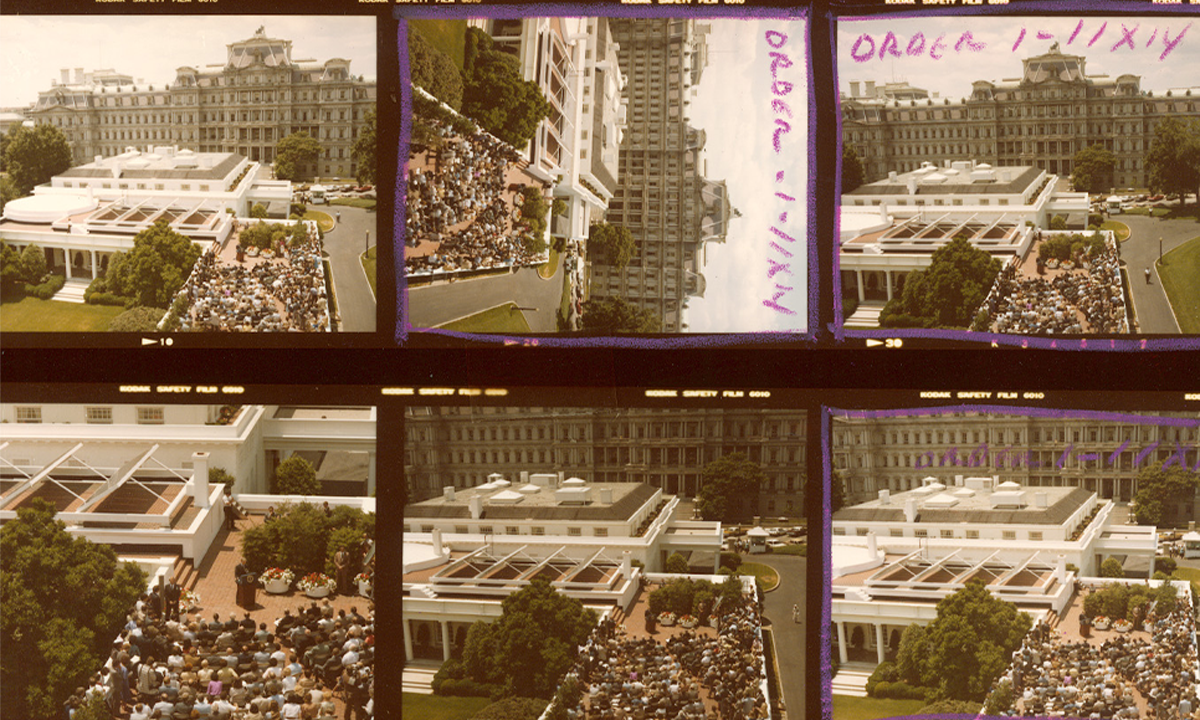
How Energy Politics Played Out on the White House Roof
The quick removal of Jimmy Carter’s futuristic solar panels echoes more recent feuds over renewables
Physics
See more PhysicsThe Science Behind the Perfect 3-Point Shot
The difference between a satisfying swish and an embarrassing air ball

Physicists Uncover How Long It Takes to Get the Last Drop of Syrup
How to tackle a common kitchen problem with fluid dynamics


Communication
See more Communication
What Would Richard Feynman Make of AI Today?
The scientific sage was always suspicious of grand promises delivered before details were understood

Get the Nautilus newsletter
Cutting-edge science, unraveled by the brightest living thinkers.
Sociology
See more SociologyThe Vibes Have Been Off in the US for Decades
New survey analysis reveals a sense of national deterioration

Does Belief in God, not Political Party, Drive Conservatism?
Religious “nones” may be less socially liberal than they used to be
Parachute Science Continues to Prevail in Global South Biodiversity Studies
The privilege of describing new species is skewed to Global Northerners
The Travels of Straight-Tusked Elephants in Europe, Written in Their Teeth
… and their travails as they encountered early humans

Read more
See all postsMoney Can’t Buy You Youth
An off-Broadway drama shows what happens when billionaires take center stage in science



Ancient People Traded Live Parrots Across South America for Thousands of Years
Polly has been wanting a cracker for millenia

Inside the Brains of Monks Who Have Meditated for 15,000 Hours
They may offer new clues to the mystery of consciousness

Were You Born to Love Music?
How you respond to art—from poetry, to visual art, to music—may be partly written in your DNA

Baby Boomers Are a Transition Generation in Our Longevity Crisis
Lifespan in the United States plateaued over a decade ago

Are You Smart Enough to Avoid Falling for “Corporate Bullsh*t”?
New research points to a troubling relationship between buzzwords and decision-making
