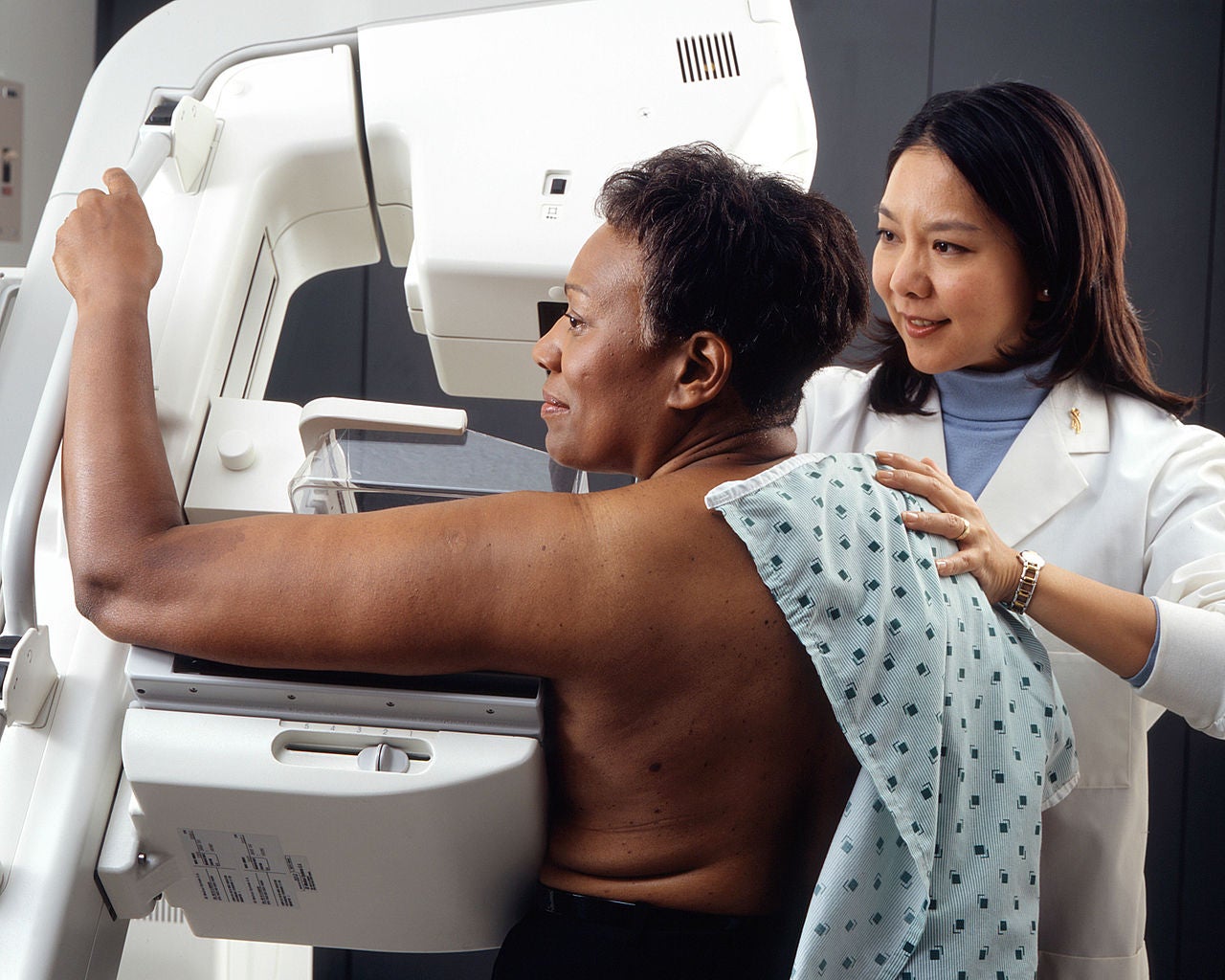
Here’s a curious fact: Black American women are 37 percent more likely to die from breast cancer than white women, according to a 2015 report by the American Cancer Society, yet they receive early-stage diagnoses much less frequently. Why might that be?
Biology’s role isn’t clear. The breast cancer death-rate in the U.S. is on the decline—from 1989 to 2012, it decreased by 36 percent, likely because, researchers suspect, treatments have improved and detection happens earlier. But that progress hasn’t benefitted everyone equally: By 2012, black women’s death-rate was 42 percent higher than white women’s. Take the case of triple negative breast cancer, a virulent type that only responds to standard chemotherapy instead of less toxic medications that target specific receptors driving the cancer, such as HER2. It’s “regularly reported to be three times more common in women of African descent and in pre-menopausal women,” according to a 2012 paper. Yet the cause of this is “unclear”—it could be a combination of genetic and environmental factors.
There is “still a high degree of segregation in primary care.”
For black women in America, these environmental factors include certain “cumulative disadvantages” that increase the likelihood of living in poverty, which may in turn limit access to adequate medical care; this can make it difficult to catch diseases in their earliest stages, when they’re the easiest to treat. Plus, the care black patients do get is often of lower quality: Numerous studies over the past few decades have found that doctors treating mostly black patients have fewer resources and tend to offer less aggressive treatment. “There’s been kind of a persistent question about disparities in care in the U.S.,” says Arden Morris, associate professor of surgery in the University of Michigan Health System. “There are many multi-pronged issues, but one of the persistent questions is: Is this a result of individual bias or systemic bias? People assume it’s a combination.”
In 2013, for example, a team led by another researcher from the University of Michigan suggested that black patients still suffer from “separate and unequal hospitalization patterns for a broad range of medical services.” They say a 2004 study’s findings help explain why: It showed that there is “still a high degree of segregation in primary care, with most black patients served by a relatively small number of lower quality physicians.” The study also concluded that physicians who take on a disproportionate amount of black patients also “reported less access to specialty resources, which suggests that they may also have trouble accessing specialist surgeons at high-quality hospitals.” Black patients themselves may not be inclined to go to the doctor in the first place—a history of patient “abuse disguised as research,” according to The New York Times, fuels mistrust of the medical establishment.
Two of the genes associated with an increased risk of breast cancer, BRCA1 and BRCA2, were discovered within the last 25 years. Normal versions of the gene suppress tumors, but mutations make women seven times more likely to develop breast cancer and 30 times more likely to develop ovarian cancer than women who don’t have it, according to the Centers for Disease Control and Prevention. (Men also have the BRCA gene, and mutations can make them slightly more likely to develop breast, skin, and prostate cancers). Doctors determine if a woman should be tested for mutations based on her family history or breast cancer diagnosis under the age of 50; if a patient opts to take the genetic test, technicians take a sample of her blood or saliva and send it to a lab. If they get tested and find out they carry the mutation, women may take steps, such as removing their breasts or ovaries, to lower their risk of developing the disease (that’s what Angelina Jolie famously did after learning she had the BRCA1 mutation).
It’s not clear how the availability of this genetic test over the last two decades has affected black-white disparities in breast cancer care. It may have had a role in increasing the incidence rate of breast cancer in black women. “Notably,” according to the 2015 report, “breast cancer rates for whites and blacks have converged in 2012, reflecting the slow, but steady increase in incidence in black women and relatively stable rates in white women.”
But the logistics of getting the BRCA test still proves to be a microcosm of these disparities. Studies have shown that doctors recommend BRCA tests less often to non-white patients. A 2011 study, for example, found that “compared to white women, black women had 75% lower odds of receiving offers of or referrals for genetic counseling, suggesting provider behavior is an important barrier to testing.” A 2016 study, published in the Journal of Clinical Oncology, had similar findings: Anne Marie McCarthy, a cancer epidemiologist at Massachusetts General Hospital, and colleagues, examined records of more than 3,000 white and black women and their 1,500 doctors to determine who took the BRCA test. The result: Both, but white patients are one and a half times more likely to do so than black patients. The discrepancy, they found, was “largely attributable to differences in physician recommendations.” That’s significant, since “one of the strongest predictors of whether women got tested is if their physician suggested it,” McCarthy says.
“I have to believe that with this many smart, dedicated people that we can continue to make improvements.”
The research team did not examine the specific reason for this discrepancy, though McCarthy speculates that cost is a factor; a 2013 study found that doctors assumed that black patients had worse health insurance or wouldn’t be able to afford the cost of the test. At about $3,000, it has been prohibitively expensive for some, and only sometimes covered by insurance. She also suspects that doctors treating black patients don’t get their full family histories, which can help determine the likelihood of carrying BRCA. Sometimes doctors don’t request such histories (there’s evidence that this happens more with black patients) but patients may also not know them, McCarthy says. And, because of “historic injustices in medical research and genetics,” according to a 2013 paper, blacks may be reluctant to seek out tests, for “fears that genetic risk information may be used by an insurer or employer to discriminate against them.”
There’s good news—at least on the cost-side of the matter. Insurance companies increasingly cover the BRCA test now that its price has dropped (in some cases it’s just $199), and the expansion of Medicaid under the Affordable Care Act means more women are insured, at least for now.
Morris, of the University of Michigan, suggests that patients bring a trusted advocate with them to doctor appointments. “If you have someone there you know is on your side, you’re going to remember that you’re there to figure out what works best for you,” says Morris, who was not involved in McCarthy’s research. That can also facilitate communication and foster greater trust between the doctor and the patient.
Ultimately, the onus seems to be on the physicians to improve the disparities among populations getting tested for the BRCA mutation, as well as for other diseases. Physicians groups and government agencies such as the National Institutes of Health are pushing for new initiatives and interventions to better support black and other minority patients. Some are testing rideshare services to help patients get better access to physicians.
For her part, McCarthy is collaborating on a recently submitted grant that will allow her to help identify patients in the healthcare system who meet the criteria for the BRCA test, offer them testing, and help them cope should they test positive. “I have to believe that with this many smart, dedicated people that we can continue to make improvements,” Morris says. “I just wish they could happen quickly.”
Image credit: Peathegee Inc / Getty