Survival of the Wittiest
How verbal humor arose and how it protects us
The Biological Basis of Imagination
Probing the mind’s eye

How Nicotine Disrupts the “Lung-Brain Axis”—And Could Lead to Dementia
Vaping might be just as bad
The Deep Secrets of the Nautilus
Evolutionary time has forged changes in these shelled cephalopods

Time Brings Order to the Universe
These scientists are proposing a new law of nature

Latest Stories



From our latest print issue
See more


Get the Nautilus newsletter
Cutting-edge science, unraveled by the brightest living thinkers.
Astronomy
See more Astronomy
Did This 17th-Century Novel Presage the Coming Artemis II Observations?
When a father of astronomy wrote the first science-fiction book about the dark side of the moon

History
See more HistoryThe Creator of the SAT Was an Infamous Eugenicist
The racist origin story of the most common college entrance exam
A Very Unscientific History of Scientific Hoaxes
The past, present, and future of academic deception
The Martyrs, Hunters, and Nature Lovers Who Came Together to Save Birds
An interview with James McCommons, author of The Feather Wars, about the past and future of bird conservation

Psychology
See more PsychologyThe Costs of Feeling Lonely in a Crowd
An interview with a loneliness researcher about the varieties of social isolation
Can Plants Count?
It seems as though they can at least track the number of events in their environment

The Students Who Believe Practice Makes Perfect Get Pretty Perfect Grades
There’s a reason it’s a popular aphorism

Get unlimited, ad-free Nautilus. Become a member today.
Environment
See more Environment
The Crowd-Sourced Science to Save Endangered Succulents
Coalescing all known information about cacti for anyone who needs to know

Ordinary Lab Gloves May Have Skewed Microplastic Data
That doesn’t mean microplastics aren’t a problem, though

Zoology
See more ZoologyWhat Happened to the Ancient Bug Giants of 300 Million Years Ago?
Insects just aren’t what they used to be



Philosophy
See more PhilosophyA Light in the Dark: Finding the Good in the Natural World
Is it absurd to think that science can inform our values?

How ‘Tiny Shortcuts’ Are Poisoning Science
Seemingly harmless data tweaks are undermining the integrity of the entire field. We must define the problem to prevent it

Doing Science and Philosophy On Drugs
Justin Smith-Ruiu takes a philosophical and first-person look at psychedelics

How Childhood Dementia Ravages the Brain
Sanfilippo syndrome is a heartbreaking disease

Read more
See all postsIs This Brain Cell the Key to Controlling Appetite?
A star-shaped support cell may have a starring role in hunger

This Record-Breaking Octopus Fossil Isn’t an Octopus After All
Uncovering a case of mistaken cephalopod identity

What Goes On Inside a Ripening Banana
The transition from green to yellow is more complicated than previously thought

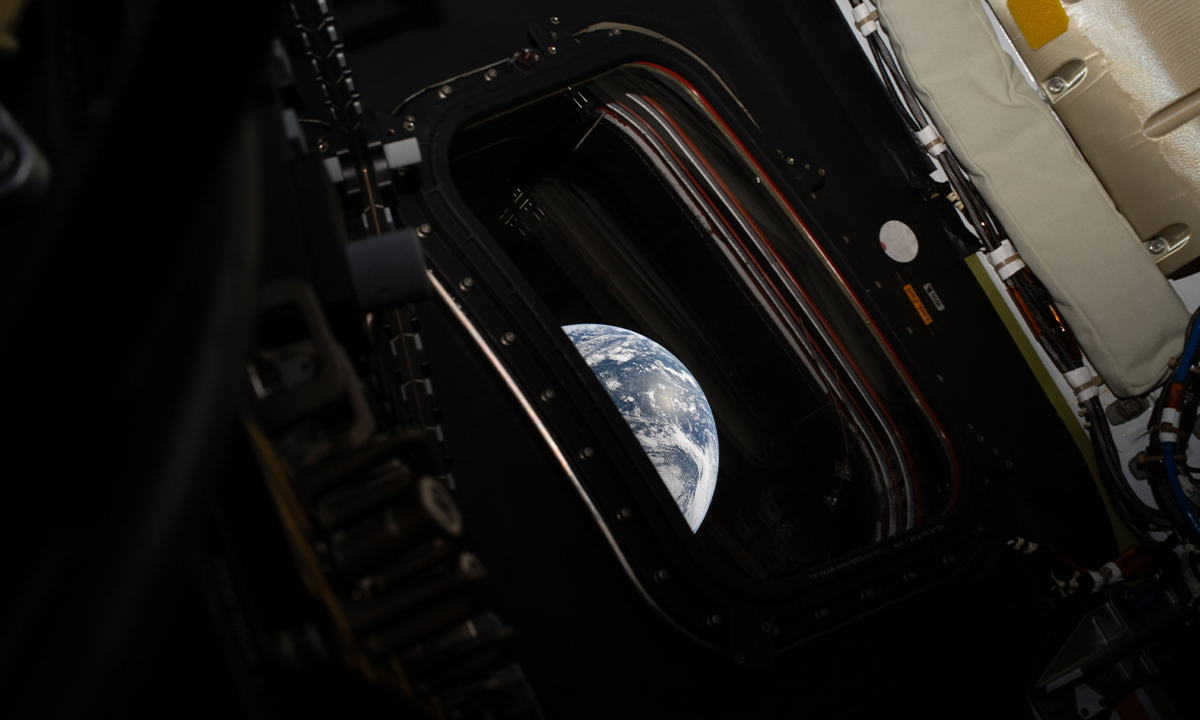
The Best Photos of the Artemis II Mission (So Far)
Humans haven’t taken photos of Earth from this distance in half a century
I Asked Claude Why It Won’t Stop Flattering Me
An interview with Anthropic’s chatbot about sycophantic AI and how to guard against it

Your Biological Clock Can be Measured With a Hair Sample
The new test opens opportunities for circadian medicine

A Poet of Science Who Shook Faith in God
Biographer Richard Holmes reveals how Tennyson predated Darwin and speaks to us today