


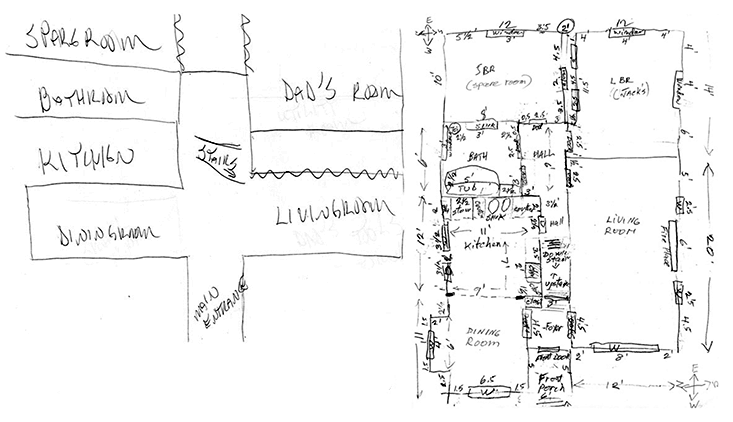
They call him “Dr. WAI,” short for “Where Am I.” A well-educated 29-year-old man without any history of disease or trauma, it took him four tries to produce a semi-accurate map of the house he had lived in for 15 years.1 Another patient, Jennifer, from San Francisco, always feels like she is facing north, regardless of which direction she is actually facing. Judy Bentley had her memory of her physical surroundings suddenly vanish one day in high school. She suddenly had no idea what was beyond the classroom door.
These are just some of the subjects that have been identified by a field that was kicked off with what might be called patient one, whom we’ll call Alice.2 In 2007, Alice approached the neuroscientist Giuseppe Iaria with a peculiar and vexing problem: She had extraordinary difficulty finding her way around. Sometimes she would even get lost in her own house. She had to rely on standardized routes, going from door to door along a carefully memorized path. To get to work she knew when to get off the bus, and how to walk from memorized landmark to memorized landmark until she reached her office building.
But if Alice strayed even slightly she would be hopelessly lost, and the only solution was to call her father to pick her up. She didn’t have any trouble seeing—she could recognize landmarks and other objects as well as anybody. Her intelligence was perfectly normal, and she was an avid reader. While she had developed a coping strategy, she was afraid it was about to fail: Her company wanted to relocate her, and she was terrified by the prospect of having to learn her way around a new environment.
Iaria, who hails from the University of Calgary, was immediately fascinated. He had spent years studying human navigation and its underlying brain systems, and knew of many subjects who had problems navigating. But all of them had some sort of brain damage, most commonly resulting from a stroke. Alice was the first person he encountered who had severe navigation problems without any apparent brain damage.
When Iaria tested Alice, he found that she fell into the normal range on a wide variety of cognitive tasks. Her brain showed no structural abnormalities, and there was no obvious problem with her upbringing that might have caused her to fail to learn how to navigate normally. She was completely unable to draw a useful map herself, though, or to form maps in her mind. The only plausible explanation, it seemed, lay somewhere in her genes. Iaria coined the term “Developmental Topographic Disorientation” (DTD) for her problem—and for other cases like her, who soon turned up in substantial numbers.
Here, out of the blue, was a new and relatively common condition that had the potential to reveal something new about how we know that we are where we are.
Let’s suppose that you are hiking in the mountains. You have a map (an ordinary paper map) and a compass (an ordinary magnetic compass); and you are trying to get to the peak of Mount Possible. There are several strategies you could use:
1. If you can see the peak from where you are standing, and see the intervening terrain, you can formulate a route based on what you see. This is “visual navigation.”
2. If you are on a trail, and there is a sign in front of you saying, “Mt. Possible 0.4 mi,” you can simply follow the trail without bothering with the map. This is “route-based navigation.”
3. If neither of those approaches are viable, you have to locate yourself on the map, use the compass to orient the map properly, locate Mt. Possible on the map, and use the map to work out a route getting you from your present location to Mt. Possible. This is “map-based navigation.”
People such as Alice generally have no problem with visual navigation or route-based navigation. Their difficulty is specifically with map-based navigation. But map-based navigation is a rather complex operation, and there are several ways it can go wrong. Some (not all) possible causes of difficulty include inability to form a good map of the environment; inability to locate yourself on your map; failure to orient yourself with respect to your map; and inability to use the map to work out a route connecting two points. Each of these failure modes probably correlates with a different type of brain dysfunction, and a different part of the brain.
Here, out of the blue, was a new and relatively common condition.
If the problem is in making a map, then the hippocampus is probably involved. Neurons in the hippocampus become active when an animal passes through specific places in the environment. These “place responses” combine information from the senses and elsewhere in the brain, particularly from the entorhinal cortex, which is located near the hippocampus and implements a spatial coordinate system.
If the problem is one of alignment, then the problem may lie with the “head direction” system, which is essentially an inertial compass located inside the brain. The hippocampus and entorhinal cortex work in close harmony with a set of brain structures implementing this system. Unlike a magnetic compass, the head direction system does not encode “true north” in any meaningful sense; instead it is more like a gyrocompass in that it uses inertial properties to maintain a consistent direction code in spite of movements and changes in orientation.
But the brain structure most frequently implicated in people suffering from damage-induced topographic disorientation is the retrosplenial cortex. This area lies near the center of the brain, and is strongly connected to the hippocampus and the other navigation-related areas. The retrosplenial cortex is not needed to have an accurate cognitive map or sense of direction, but it seems somehow to be crucial, in a way we don’t yet understand, for the ability to properly use the map and compass to formulate a route to a goal.

The underlying causes of DTD probably include some or all of these possibilities. Some people, such as the initial patient, Alice, seem to form cognitive maps that are severely distorted: This suggests a dysfunction in the entorhinal cortex or parietal cortex, the areas that are involved in grasping spatial relationships. For others, the difficulty centers on orientation, suggesting a dysfunction involving the head direction system. Judy Bentley, one of Iaria’s patients, finds her sense of direction to flip unpredictably between four settings, and each time it flips she has to learn a new set of relationships. Sharon Roseman also frequently loses her sense of direction, but she has learned that if she closes her eyes and spins around, upon opening her eyes it usually comes back. And Jennifer, the San Franciscan patient, always feels like she is facing the same direction, even as she turns from side to side.
The few systematic experimental studies of DTD that have been done implicate certain structures and functions of the brain, but are not conclusive. Two years ago Iaria and several colleagues found reduced interactions between the hippocampus and prefrontal cortex in nine women suffering from DTD, compared to control subjects. That’s interesting, but there are reasons to suspect it might be a consequence of DTD rather than a cause: To put it crudely, the hippocampus makes maps and the prefrontal cortex makes plans—reduced interactions suggest that the plans people make are less influenced by their maps. This may simply be a result of people having learned that their maps are unreliable.
The odds are high that some of the readers of this article suffer from DTD, and don’t know it.
In a 2014 paper, a group of investigators from Princeton and Carnegie Mellon University did a thorough study of brain activity in a woman with DTD who was asked only to view spatial scenes on a computer screen, not to actually navigate.3 When her brain activity patterns were compared with those of control subjects, no differences were seen for the hippocampus, but clear differences appeared for the retrosplenial cortex—the same brain area most often affected in topographic disorientation caused by brain damage. The subject showed reduced effects of familiarity on her retrosplenial responses, and reduced functional connectivity between the retrosplenial cortex and the “parahippocampal place area,” a portion of the temporal lobe involved in encoding memory for scenes. Thus it is possible that the retrosplenial cortex will turn out to be as critical for DTD as it is for brain-damage-caused topographic disorientation—at least in some cases.
Over the long term, perhaps the most important information DTD might give us will be a better understanding of the genes involved in spatial cognition. There is anecdotal evidence that DTD is often inherited—Iaria promises to publish a paper soon that will back up that claim—and if it is possible to identify a small number of genetic variants that distinguish people with DTD from others, we will have an excellent start. It might not work: The number of genes expressed specifically in the brain is huge, and there is no telling how many are involved in spatial cognition. Unless multiple people with DTD show mutations of the same genes, it will be difficult to make progress. But it is certainly worth trying. The results would not only be useful for understanding DTD, they would also potentially be useful for understanding the normal range of variation in spatial abilities. Where large mutations cause severe problems, smaller differences in gene expression are likely to cause more moderate differences in behavior.
A particularly intriguing point, in relation to the genetics of DTD, is that it seems to show up much more often in women than men: Iaria’s initial group of 120 subjects included 102 women and 18 men.4 This doesn’t amount to proof, because most of Iaria’s DTD cases were self-reported, and women could simply be more open about this problem than men. To properly establish a relationship would require a randomly selected sample of people. Even so, the difference is large enough that it can be expected to hold up, especially given that studies have shown that, on average, men are a little bit better than women at map-based navigation.5 Thus at least some of the genes in question are likely to show sexually dimorphic patterns of expression.
Over the last five years, several hundred cases of DTD have been identified. It might actually not be uncommon: An informal survey that Iaria carried out among students at the University of Calgary found that as many as 2 percent of them might meet the criteria for the disorder. The odds are high that some of the readers of this article suffer from DTD, and don’t know it. Iaria plans to have an online test available for the public this July. It may very well be worth taking. As for Alice, she ended up not being relocated, and continued to find her way to her old job one landmark at a time.
William Skaggs is a neuroscientist and science writer, whose research has focused on the role of hippocampus in spatial cognition and memory.
References
1. Bianchini, F., et al. Where am I? A new case of developmental topographical disorientation. Journal of Neuropsychology 8, 107-124 (2014).
2. Iaria, G., Bogod, N., Fox, C.J., & Barton, J.J. Developmental topographical disorientation: Case one. Neuropsychologia 47, 30-40 (2009).
3. Kim, J.G., Aminoff, E.M., Kastner, S., & Behrmann, M. A neural basis for developmental topographic disorientation. The Journal of Neuroscience 35, 12954-12969 (2015).
4. Iaria, G., & Barton, J.J. Developmental topographical disorientation: A newly discovered cognitive disorder. Experimental Brain Research 206, 189-196 (2010).
5. Andersen, N.E., Dahmani, L., Konishi, K., & Bohbot, V.D. Eye tracking, strategies, and sex differences in virtual navigation. Neurobiology of Learning and Memory 97, 81-89 (2012).









